HEART RHYTHM SPECIALIST

Atrial Fibrillation: Which treatment strategy?
Drugs or AF Ablation or Ablate and Pace?
The following presentation covers the various treatment options for AF in detail. Please click Atrial fibrillation treatment options.ppt
Drug therapy for Atrial Fibrillation
Some examples of the drugs used to control AF are Sotalol, Flecainide, Dronedarone and Amiodarone.
Although simple to institute for the doctor, and easy to take for the patient, there are some potential disadvantages of drug therapy:
-
•treatment needs to be continuous, often life-long, as drugs don’t cure AF but merely keep it at bay
-
•most drugs are associated with side effects, and some of these can be serious. Also in the case of Amiodarone, the side effects are cumulative, i.e., the risk increases with time
-
•the drugs may become less and less effective over time, so that either different drugs need to be tried or more than one drug is needed.
Catheter Ablation for Atrial Fibrillation
This is a relatively new treatment, and has only become part of mainstream medicine for the last 10 years or so. In this the cardiologist uses Radiofrequency energy to create electrical lines of block in the heart so that the triggers for AF are abolished. In the more advanced cases of persistent AF, a more extensive lesion set may be needed. This is done via tubes inserted in veins at the top of the leg, and patients are on their feet and out of hospital the following day.
The advantage of catheter ablation is that it targets the underlying triggers for AF and so has a potential for curing the condition, rather than just controlling it. The main disadvantage is the 2-3 in 100 risk of potential complications associated with the procedure. Besides, as this is a highly specialised technique, it is only available in a handful of centres. For instance, as of 2013 there are less than 100 cardiologists performing this procedure in the UK.
So, which of the two is better?
There are a number of head- to-head comparisons in scientific literature, and ALL of them have shown that Catheter ablation is superior to drug therapy (see figure below).
What about Ablate and Pace treatment?
This involves disconnecting the atria from the ventricles by ablation of the AV node, and implanting a permanent pacemaker to support the function of the ventricles. It can relieve AF symptoms due to fast erratic heart beat, but doesn’t cure the underlying AF. This treatment has been used for the very elderly patients and often as a last resort when all other options have failed.
There are a number of concerns around this treatment:
-
•It doesn’t cure the underlying problem, but merely ‘hides’ it from view. The AF continues unabated, as do its deleterious effects of loss of atrial contraction and the risk of clot formation.
-
•The patient is left with no underlying heart rhythm, and is dependent on a pacemaker all his/her life. Any pacemaker malfunction/infection etc can have catastrophic consequences.
-
•A number of studies have now shown that continuous pacing can weaken the heart over time and cause heart failure.
-
•The ideal goal in medicine is to restore normal physiology as far as possible. (‘Nature is best’). The Ablate and Pace treatment is the very antithesis of this.
-
•The AV node ablation is irreversible and can not be undone. This means that these patients can not benefit from any future advances in the curative ablation treatment for AF.
Due to these reasons, doctors are increasingly reluctant to offer this treatment to AF patients, and Dr Gupta is delighted with this trend. If your doctor is considering this treatment for you, please make sure that you understand all the long term implications of this fully.
In Dr Gupta’s opinion, advanced age alone should no longer be considered a valid reason to advise an Ablate and Pace strategy in favour of AF ablation, especially for patients suffering from Paroxysmal AF. The results of AF ablation in the elderly are now very encouraging. (see ‘Satisfied Patients’ section)
Some patients in whom Ablate and Pace treatment may still have a place are:
-
•Elderly patients (>75-80 years) with long standing persistent AF or in whom AF ablation is likely to be unsuccessful/ too risky on account of anatomical reasons. For example, patients with very large left atrial size or say those with artificial heart valves.
-
•Patients whose predominant symptom is palpitations, and not breathlessness or fatigue.
-
•As a last resort in patients in whom AF ablation attempts have been unsuccessful as well as all forms of drug therapy. This should form a small minority of patients in this day and age.
References:
-
1.PVI vs Ablate and Pace for elderly patients with paroxysmal AF. J Cardiovasc Electrophysiol 2005; 16: 457-61.
-
2.PVI, Ablate and Pace, and DC cardioversion with antiarrhythmic drugs: survival rates at 7 years follow up. J Interv Card Electrophysiol 2009; 26:121-126
So if AF ablation is the most ideal treatment, what do I need to know about it?
For Q&A about AF ablation, see here
Ref: Why Atrial Fibrillation Ablation should be considered first line therapy for some patients.
A Verma, A Natale
Circulation 2005;112:1214-1231
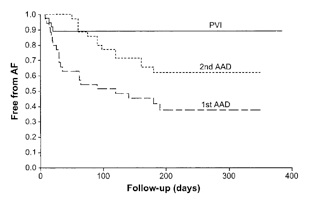
Key
PVI: Pulmonary vein isolation/ Ablation
AAD: Anti-arrhythmic drug therapy
